This module primarily offers educational materials and pedagogical tools for professionals who train healthcare professionals working with individuals affected by domestic violence (DV) in their daily practice. It is intended exclusively for professionals in this sector and not designed for individuals experiencing DV or those in their immediate social environment.
Brief overview of Module 3
Module 3 provides an overview of “communication in cases of domestic violence (DV)”. This module presents the critical aspects of communication when addressing DV. Understanding the complexities related to disclosure, employing effective communication strategies, and crafting appropriate responses are paramount in providing comprehensive support to victims of DV. Specific information on communication in the medical sector, and how to better support victims with a focus on gynaecology/obstetrics, the emergency room (surgery), paediatrics, and dentistry, is also included.
The objectives trainers can address with the materials of Module 3 are as follows:
+ Help trainees gain a better understanding of the existing barriers that may prevent individuals from disclosing DV. + Enhance trainees’ ability to apply visual communication methods to facilitate communication in cases of DV. + Enable trainees to use screening questions to identify cases of DV. + Equip trainees with communication strategies tailored to the specific challenges of DV cases. + Guide trainees in responding appropriately and empathetically to disclosures of DV, ensuring that victims feel supported and understood. + Deepen trainees’ understanding of the next steps to take when victims disclose violence.
1. Barriers to Disclosure
Individuals experiencing domestic violence may face various challenges that can make it difficult for them to openly discuss their situation.
Please click on the crosses in the corresponding circles below each term in the illustration to see further information on some common barriers:
Please remember:Victims of domestic violence come from all social, cultural, economic, and religious backgrounds with different age, gender and sexual orientation, including people with disabilities. It affects people from all socio-economic backgrounds and education levels. It is important to understand, that there is NO “typical victim”.
Even though many example videos depict a female as the victim in heterogenous relationships, please do not be misled. Victims can be anyone, including men, children, individuals with disabilities, or non-binary persons. The same applies to perpetrators. For more information on perpetrators, check out Module 1. Also, domestic violence can occur between couples, same-sex couples, parent and child, siblings, uncles, aunts, cousins, grandparents or even roommates.
2. Communication Strategies
To foster a respect- and trustful communication about the experienced violence, ensure victims have a private spacewithout accompanying individuals (partner, children, other family members or non-family caretakers) allowing the patient to speak freely and comfortably. In general, it is useful to use “I-Messages”. It can be used specifically to solve ambivalences in a victim during the counselling or in case of less time for counselling.
“Never assume and always ask!”
The Royal Australian College of General Practitioners (RACGP)1
Please click on the crosses in the corresponding circles below each term in the illustration to see further information.
Perpetrators usually accompany victims to the hospital or doctor´s visit. They don´t want the victim to be all alone with the health care professional. The challenge is to mange to see the patient alone and not making the perpetrator angry and increase the risk for escalation of DV later.
Here are some suggestions how this can be done:
Ask the accompanying person to fill out additional paperwork
Explain to the accompanying person e.g. in the emergency room that radiologic exams may be necessary with a high risk of x-ray exposure and due to safety concerns he/she is not allowed into the examination room.
Explain that hospital policy does not allow accompanying the patient during the exam. The following video is a good example on how to communicate this well:
Patient Cues and Empathetic Listening
“Patients often present clues (direct or indirect comments about personal aspects of their lives or their emotions) during conversations with their physicians. These clues represent opportunities for physicians to demonstrate understanding and empathy and thus, to deepen the therapeutic alliance that is at the heart of clinical care.”2
“Empathetic listening requires understanding how to recognise the cues that patients offer. There are opportune moments for verbal responses to what the patient is sharing. Cues might be a decrease in emotional intensity, a deep sigh, or a shift in the focus of the conversation. At this point, it may be natural to respond to their message and attend to the medical care needed. Verbal reflection may be helpful for conveying empathy when you need more description or explanation from the patient, or when you sense the patient would like confirmation that you are listening and understanding.”3
How can I use body language to show empathy right away? 4
> Sitting next to or near the patient > Leaning in their direction > Maintaining eye contact > Making sure your arms are not crossed > Not focusing solely on a computer keyboard or screen with your back to the patient > Periodically echoing or summarising what the patient is saying
> Interrupting or finishing the patient’s sentences > Challenging the patient’s feelings > Speaking in a manner that sounds patronising > Describing what the patient ought to think or feel > Lack of emotional acknowledgement by changing the topic and proceeding with medical questions
Case study: Disclosure of domestic violence in medical practice
Mr. Thompson, an 80-year-old widower, sought medical attention for anxiety and signs of depression.
Dr. Miller: Good morning, Mr. Thompson. How are you feeling today?
Mr. Thompson: Oh, you know, just the usual aches and pains that come with age. Nothing much to worry about.
Dr. Miller: I understand. But I’m here to help with any concerns you might have. Anything on your mind that you’d like to discuss?
Mr. Thompson: Well, doc, it’s not just the physical stuff. I’ve been feeling down and tired lately.
Dr. Miller: I appreciate your openness, Mr. Thompson. Let’s talk about anything that might additionally be on your mind. Besides the physical discomfort, have there been any changes in your life or relationships that might be affecting your well-being?
Mr. Thompson: (hesitant) It’s… it’s not easy to talk about. But it’s Jessica, my caregiver. Things haven’t been great.
Dr. Miller: It takes courage to discuss difficult situations. Can you share more about what’s been happening?
Mr. Thompson: She gets angry a lot, and there are hurtful words. I feel like I’m walking on eggshells, you know?
Dr. Miller: I’m sorry to hear that, Mr. Thompson. It sounds challenging. Can you share more about how it’s affecting you?
Mr. Thompson: (guarded) It’s affecting my sleep, my mood. I feel trapped in my own home.
Dr. Miller: Thank you for trusting me with this information.
Mr. Thompson: I just want it to stop, doc. It’s affecting my health, both physically and mentally.
Dr. Miller: I hear you, and I’m here to help. We can work together to address these concerns. If you’re comfortable, we may need to involve others to support you.
Mr. Thompson: Thank you, doc. I… I didn’t know if I should say anything. It’s just been hard. I didn’t know where else to turn.
Dr. Miller: You’re not alone in this, Mr. Thompson. We’ll take steps to ensure your safety and well-being, involving the right people to support you through this difficult situation.
Task for reflection
(1) Examine the role of trust-building in this case study. How did Dr. Miller establish trust with Mr. Thompson, considering the sensitive nature of the situation? Reflect on strategies for building trust in challenging and vulnerable circumstances.
(2) Identify specific cues Mr. Thompson gave during the consultation that hinted at potential domestic violence. How did Dr. Miller recognise and interpret these cues?
Of note: Although this video is from the U.S., its content applies to European realities. For further information see Module 2 and the impact of DV.
“Trauma-informed primary care can transform the caregiving experience of providers from being treaters to being healers.”
Eddy Machtinger, MD, Director of Women’s HIV Program, UCSF
“Trauma-informed care shifts the focus from “What’s wrong with you?” to “What happened to you?” A trauma-informed approach to care acknowledges that health care organisations and care teams need to have a complete picture of a patient’s life situation — past and present — in order to provide effective health care services with a healing orientation. Adopting trauma-informed practices can potentially improve patient engagement, treatment adherence, and health outcomes, as well as provider and staff wellness.” 6
Seeking Care After Trauma: Challenges in Booking a Gynecologist After Rape (The Klingenbeck Case)
This video follows a person who has experienced rape as they navigate the process of finding a new gynecologist. It illustrates the fears, thoughts, and emotional barriers that can arise when seeking medical care after trauma. Through their inner dialogue and hesitation, the video demonstrates how past experiences can impact access to essential healthcare and emphasises the importance of sensitive, trauma-informed support from medical professionals.
Task for reflection
(1) What are the main barriers the person experiences when trying to make a gynecologist appointment? (2) In what specific ways does past rape affect the person’s trust in medical professionals? (3) Why is trauma-informed care in a clinical setting so important?
3.2. Patient-Centred Care
Patient- and family-centred care promotes active partnership and joint decision-making among patients, families, and healthcare providers to formulate and oversee a tailored and comprehensive care plan. Several key components shared by most definitions of patient-centred care shape the design, management, and delivery of healthcare services: 8
Collaborative, well-coordinated, and easily accessible care, ensuring the right care is delivered at the right time and place.
Information is shared fully and in a timely manner so that patients and their family members can make informed decisions.
“The patient’s goals need to be considered as part of the healthcare plan, rather than an assumption or prescription of what the goals should be (this is consistent with trauma-informed care).” 9
“A patient’s current and past health status, and relevant information affecting health, including trauma, need to be considered in care planning and delivery.” 10
“A patient needs to be able to obtain quality care when and in the ways, they need it, not just in a single model of care.” 11
3.3. Gender-sensitive language
“Many transgender and gender-diverse (TGD) people make changes to their name, pronouns, and physical appearance to affirm their gender identity. It is not possible to know someone’s gender identity based on their name, appearance, or the sound of their voice. Using the wrong name, pronoun, or gender can cause embarrassment and humiliation for anyone, not just TGD people. Men with high voices are often called “ma’am” on the phone. Women with short hair are often called “sir.” For TGD people, being misgendered like this is common and can be very distressing.” 12
Creating a gender-affirming experience begins with communication. Use these best practices as a guide to ensure respectful and appropriate interactions with patients: 13
Best Practices
Examples
When addressing patients, avoid using gender-specific terms like “sir” or “ma’am”
“How may I help you today?”
When talking about patients, avoid pronouns or other gender-specific terms. If you have a record of the name used by the patient, use it in place of pronouns.
“Your patient is here in the waiting room.” “Max is here for a 3 o’clock appointment.”
Politely ask when you are unsure about a patient’s name or pronouns used.
“What name do you go by, and what are your pronouns?” “I would like to be respectful. How would you like to be addressed?”
Ask respectfully about names when they do not match the one you have in your records.
“Could your chart be under another name?” “What is the name on your insurance?”
Did you use the wrong pronoun? Politely apologise.
“I apologise for using the wrong pronoun. I didn’t mean to disrespect you.”
Only ask information that is necessary for providing care.
Ask yourself: What do I know? What do I need to know? How can I ask in a sensitive way?
Case study: Disclosure of domestic violence of a transgender women in medical practice
Below is an example of a positive patient-staff interaction. The scene presented here is between Claire, a transgender woman, and Danielle, a front desk receptionist.
Danielle: Good afternoon. How may I help you?
Claire: Hello. I have an appointment with Dr. Brown at 2:30.
Danielle: Your name please?
Claire: Claire Brooks.
Danielle: I’m sorry but I don’t have you listed here. Might your appointment be under a different name?
Claire: Oh yes. I changed my name recently from Lawrence to Claire.
Danielle: Okay, I see here that the appointment is under Lawrence Brooks. I’m sorry for the mistake. I will update our registration system right away with your correct name.
Just to be sure we are using the right records; would you be able to tell me your birth date?
Claire: November 12, 1987.
Danielle: Great. And have you changed your name on your insurance?
Claire: No I have not.
Danielle: Okay, thank you. Just so you know, I won’t be able to change the name on your insurance for you. However, we have a case manager here who helps people with insurance and legal needs. Do you want me to get you in contact with her?
Claire: Oh yes, that would be great. Thank you.
Danielle: Sure thing.
Task for reflection
(1) In this scenario, Danielle uses several communication strategies with Claire. Can you identify what they are?
It is crucial to inquire about domestic violence through screening questions without exacerbating the risk of harm to victims and their children. The screening process should commence with a framing statement to introduce and normalise the questions, such as: “I have some questions that I ask every patient. I’m going to ask you these questions now, too.” 14
Every effort should be made to screen in the patient’s preferred language in case of language difficulties , and cultural barriers should be recognised during the screening process.
Pose behavioural questions that solicit descriptions of behaviour rather than solely focusing on the impact or meaning of behaviours.
Present questions in a calm, matter-of-fact manner. In cases where responses are unclear, briefly seek further clarification through additional questions.
Always express gratitude for the provided information 15
Remember: Explore different approaches to discover the one that suits you best, recognising that each patient may respond differently to various methods.
Start with asking general questions
Use statements like these to raise the subject of violence before you ask direct questions. Open questions should be asked to encourage the victim to talk instead of saying yes or no. Avoid questions that put the blame on the victim.
Good to use
“How are things at home?”
“How do you get along with your partner?”
“I know many people have problems facing violence by their partners, other family members, or someone else they live with. Could it be, that this is the same in your case?”
Do not use
“Do you experience domestic violence?”
“Has someone close to you used you as a victim?” 16
Framing the question
Create space for silence, allowing the individual time to gather their thoughts. Demonstrate patience and maintain a calm demeanour. Signal your attentive listening, whether through nodding or verbal cues like “hmm….”. Validate the emotions and encourage the patient to share the story at a pace that feels comfortable for them.
Good to use
“Because unfortunately violence is so common in our society, I have started asking all of my patients about it.”17
“I’m going to ask you a question that I ask all patients.”
“Because domestic violence has so many effects on health, I now ask all my patients about it.” 18
More examples
“From past experience with other patients, I’m concerned that some of your medical problems may be the result of someone hurting you. Is that happening?”19
“I don’t know if this is a problem for you, but many of my patients are dealing with abusive relationships. Some are too afraid or uncomfortable to bring it up themselves, so I’ve started asking about it routinely.”20
“Violence affects many families. Violence in the home may result in physical and emotional problems for you and your child. We are offering services to anyone who may be concerned about violence in their home.“ 21
Do not use
“I am asking you about violence because only women are victims.”
Ask direct questions
Here are some simple and direct questions that you can start with. They show you want to hear about their problems. Depending on their answers, continue to ask questions and listen to their story. If they answer “yes” to any of these questions, offer support. Do not tell the victim it is not that bad or minimise the pain.
Good to use
“Are you ever afraid at home or in your relationship?”
“Has your partner or someone else at home ever threatened to hurt or physically harm you in some way? If so, when has it happened?”
“Does your partner or someone else at hometry to control you, for example not letting you have money or go out of the house?”
More examples
“Have you been pressured or made to do anything sexually that you did not want to?”22
“Have you been hit, kicked, punched, or otherwise hurt by someone within the past year? If so, by whom?”
“Do you feel unsafe in your current relationship?”23
“Is there a partner from a previous relationship who is making you feel unsafe now?”24
“Have you ever felt controlled or isolated by someone close to you?” 25
“Do you have a safe place to go in an emergency?”26
“Does your partner or someone else at home ever try to control you by threatening to hurt you or your family?”27
“Have you ever been slapped, pushed or shoved by someone close to you?”
Do not use
“Why are you still living with your partner/family member who treats you like that?”
Opting to reveal experiences of domestic violence is an individual choice, and DV victims may opt not to communicate about it with healthcare professionals for various reasons, such as concerns for safety, fear of potential consequences, or a lack of trust, among others. In the event of a patient disclosing domestic violence, employing a patient-centred approach proves beneficial in offering support to the individual and their family. Healthcare professionals can act as advocates for domestic violence victims, drawing on their resilience and strengths. 29
Description: The video illustrates how one should respond to a disclosure in cases of domestic violence.
When someone opens up, listen actively without judgment or offering solutions, giving them the space to express their needs. While you can seek clarification through questions, focus on allowing them to share their emotions. Pay attention to both spoken and unspoken cues, and use the following techniques to help them articulate their needs, ensuring a better understanding.
Empower the individual
The victim should be helped to identify and express their needs and concerns. Allow silences. If the individual cries, give enough time to recover.
No “why” questions should be asked.
Phrases to use
“When you said earlier that your partner/family member lashes out at you [or whatever behaviour they’ve described], I’m wondering if you can tell me what that means?”30
“Is there anything you need or are worried about?”
Do not use/do
“Why did you do that?”
“Why did you upset your partner/family member?”
Don’t try to finish the thoughts for the individual. 31
Building trust and showing empathy
Ensure clarity in communication by repeating what the victim has shared to confirm your understanding. Reflect the emotions conveyed by the victim and summarise their expressed concerns. Avoid using suggestive questions during the conversation.
Phrases to use
“You mentioned that you feel very frustrated.”
“It sounds as if you are angry about this…”
“You seem to be saying that…”
Do not use/do
“I imagine that upsets you, doesn’t it?”
Don’t look at your watch or speak too rapidly. Don’t answer the telephone, look at a computer or write. 32
Validate feelings
Assure the other person that their emotions are typical, create an environment where it’s secure to share those feelings, and emphasise their entitlement to a life free from violence and fear. Validation involves expressing attentive listening, comprehension, and belief in what they communicate without passing judgment or attaching conditions.
Phrases to use
“It’s not your fault. You are not to blame.”
“It’s okay to talk.”
“Help is available.” [Say this only if it is true.]
More examples
“There is no justification or excuse for what has happened.”
“No one deserves to be hit by their partner or other family member in a relationship.”
“You are not alone. Unfortunately, many other people have faced this problem too.”
“Your life, your health, you are of value.”
“Everybody deserves to feel safe at home.”
“I am worried that this may be affecting your health.”
Do not use
“Stop feeling so bad, it could be worse”
“This feelings will go away, do not worry.”
Offer support
Assure you are not judgemental. Don’t advise things. Signalise that there is no excuse for violent behaviour. Take the victim seriously. Be empathetic. Appreciate the victim’s experiences. Assist the individual in recognising and articulating their needs and concerns
Phrases to use
“I know this is difficult to discuss, but you can talk to me.“
“You are not alone. I’m here for you.“
“You are not responsible for what’s going on.“
More examples
“Violence is never ok and you do not deserve it.“
“Thank you for trusting me and sharing your feelings.”
“Is there anything that you
need or are concerned about?
Do not use/do
“You should definitely get divorced”.
“I believe this conforms to typical ‘men’/’women’ behaviour, and there’s no need to overreact.”
Don’t tell the person someone else’s story or talk about your own troubles.33
Avoid confrontation
If the victim is not ready to talk about the situation, do not force it. Recognise the right time and let the victim know about it. Lay off the pressure.
Phrases to use
“I’m here to help, and I’m available, even if I understand that you don’t want to talk about it now.“
“Remember that you’re not alone. I’ll be here for you when you’re ready.“
Do not use
“Even though you feel uncomfortable, it is better to talk about it. So please answer my questions.”
Let the individual make their own decisions
Avoid judging the victim’s ability to make decisions, thus preventing that she/he loses confidence in you. Encouragement and asking is the key.
Phrases to use
“What can I do to support you?“
“How can I help to protect your safety?“
Do not use
“If I were you, I would go to the police and file a report“
Provide ways to get help
Let the individual know about specialist family violence services that can offer professional support. Avoid convicting or condemning statements.
Phrases to use
“Here is the number to your local domestic violence office. They can help with shelter and counselling.“
“Do you want me to help you develop a safety plan?“
“I want to help you (your child, etc.) be healthy and also safe. I want to share these resources I give to all of my patients. I give everyone two of them so you have the info for yourself and you can give one to a friend. We all know someone who’s struggling and may need support.”
Do not use
“You should definitely call this number and leave the perpetrator immediately!”
“Why didn’t you leave this person long ago?”
“If you would have come earlier, I could have helped you better”.
If there is a legal case in the future, you as a medical professional may be questioned about the victim, so you should document everything well. Find further information in Module 4: Medical assessment and securing of evidence.
Find more information about the criminal processes involved after reporting to the police here.
Case study: Disclosure of domestic violence in medical practice
A 19-year-old patient visits a family practice for a consultation.
Physician: “Good morning, what can I do for you today?”
Patient: “I feel totally overworked at the moment and wanted to ask if you could put me on sick leave for two weeks?”
Physician: “Is there any particular reason why you feel that way and has this happened before?”
Patient: “I have never been on sick leave because of overload before. But I recently moved out of my parents’ house in my own flat. Everything just gets too much for me at the moment.”
Physician: “Of course, I can put you on sick leave, but if you feel so overwhelmed by your situation, I would be happy to offer you further support. Perhaps you would like to talk to me about it?”
Patient: “Mmm, I actually feel very uncomfortable to talk about it. There were some problems with my mother in the past. She is a control freak and constantly checked my cell phone. We were fighting whenever I wanted to meet with my friends or family. As a result, I became more and more isolated and the only company when leaving the house were my parents. My mother read messages from my friends before I had a chance to read them. I felt very bad that’s why I decided to move out. But I don’t know if that was the right decision.”
Physician: “If your mother controlled and bullied you so much, why do you think to move out was a mistake?”
Patient: “During the time living in my own flat now, my mother kept calling me and sending me messages. I feel under pressure by saying that she cannot live without me and will hurt herself if I don’t come back. I see her car in the parking lot all the time: while shopping, being at work or meeting my friends. I always have the feeling that she is around. Can that even be a coincidence? I have already met her many times because I felt so sorry for her, and I was afraid that she would really hurt herself.”
Task for reflection
(1) Reflect on the physician’s response to the patient’s initial request for sick leave. How did the physician show empathy, and what cues in the patient’s language indicated there might be an underlying issue?
(2) Consider the moment when the patient hesitated to talk about the problems in the relationship. How manage the physician to enhance trust and to create a safe space for the patient to share the experiences?
(3) Analyse the patient’s description of the relationship with the mother. What are the red flags or signs of potential domestic violence? (see also Module 2)
6. Questions that often arise in the context of DV
Here are answers to some questions that might come up for health-care providers working with victims subjected to domestic violence.34
“What can I do when I have few resources and little time?”
It does not necessarily take long, and it does not require additional resources: sometimes, one sentence is enough to let the victim know that they are not alone, that violence is never an option and that they can get help if they want to. Also, you can learn about resources in the health-care system and in the community that can help them.
“Why not offer advice?”
It is important for victims to be listened to and to have an opportunity to tell their story to an empathetic person. Most victims do not want to be told what to do. In fact, listening well and responding with empathy is far more helpful than you may realise. It may be the most important thing you can do. Victims need to find their own path and come to their own decisions. Talking about it can help them do this.
However, information (e.g., via pamphlets) on available resources (e.g., financial support, contact data of shelter) should be offered.
“Why do they not just leave them?”
There are many reasons for victims to stay in violent relationships. It is important not to judge them and not to urge them to leave. They have to make that decision themselves, in their own time. Reasons for not leaving include:
Financial/social etc. dependence can be experienced. Some individuals rely on their caregivers.
Some individuals may think that violence is normal in relationships and that all partners/family members will be violent and controlling, believing they deserve it.
Fear of an extreme and violent reaction to leaving.
Feeling there’s no place to go or no one to turn to for support.
Find more information on the dynamics of domestic violence in Module 2.
“How did they get themselves into this situation?”
It is important to avoid blaming the victim for what happened. Blaming the victim will get in the way of your giving them good care. Violence is never appropriate in any situation. There is no excuse or justification for violence. No one ever deserves to be hurt.
“That wasn’t the way we were taught.”
Health-care providers are generally taught that their main role is to diagnose the problem and treat it. However, in this situation limiting the focus to medical concerns is not helpful. Instead, you need to add a human focus by listening, identifying victim’s needs and concerns, strengthening their social support, and enhancing their safety. Also, you can help them see and consider their options and help them feel they have the strength to make and carry out important decisions.
“What if they decide not to report to the police?”
Respect their decision. Let them know that they can change their mind. Let them know that there is someone they can talk to about their options and help them make the report if they choose to.
“How can I promise confidentiality if the law says I have to report to the police?”
If your law requires you to report violence to the police, you must tell the person this. You can say, for example, “What you tell me is confidential, that means I won’t tell anyone else about what you share with me. The only exception to this is…”
As a health-care provider, learn about the specifics of the law and conditions in which you are required to report (for example, the law may require reporting rape or child abuse). Assure them that, outside of this required reporting, you will not tell anyone else without their permission. Find further information on legal aspects in different countries in Module 7.
“What if they start to cry?”
Give them time to do so. You can say, “I know this is difficult to talk about. You can take your time.”
“What if I suspect violence but they do not acknowledge it?”
Do not try to force them to disclose. (Your suspicions could be wrong.) You can still provide care and offer further help.
“What if they want me to talk to their partner/family member/caregiver?”
It is not a good idea for you to take on this responsibility. However, if the victim feels it is safe to do so and it will not make the violence worse, it may be helpful for someone they respect to talk to them – perhaps a family member, a friend, or a religious leader. Warn them that if this is not done carefully, it could lead to more violence.
“What if the partner/family member/caregiver is one of my client, too?”
It is very hard to keep seeing both individuals when there is violence in the relationship. Best practice is to try to get a colleague to see one of them, while ensuring that confidentiality of the victim’s disclosure is protected.
“What if I think their partner/family member/caregiver is likely to kill them?”
Share your concerns with the victim honestly, explain why you think they might be at grave risk and explain that you want to discuss possible options for keeping them safe. In this situation identifying and offering secure alternatives where they can go is particularly important.
Be prepared for such a situation and have a leaflet with respective telephone numbers (e.g., from a shelter) at hand. Make sure this list is up to date.
Ask if there is a trusted person you can include in the discussion and whom you can alert to the risk.
“What if I cannot handle what I hear?”
Your needs are as important as those of the victim you are caring for. You may have strong reactions or emotions when listening to or talking about violence with victims. This is especially true if you have experienced abuse or violence yourself – or are experiencing it now. Be aware of your emotions and take the opportunity to understand yourself better. Make sure to get the help and support you need for yourself.
7. Communication within Healthcare Teams
Challenges with colleagues or structural barriers regarding the topic of domestic violence can arise, especially in the hectic routine of a hospital or medical practices. Unfortunately, there are instances where support may not come from colleagues or higher-ups when dealing with domestic violence, because they do not wish any involvement, are unaware of their obligations or they do not have the proper training.
In this video, a healthcare provider engages in a conversation emphasising the significance of implementing the safety card intervention with a hesitant colleague.
Task for reflection
(1) Evaluate the effectiveness of communication strategies used in the video. Reflect on the importance of clear and empathetic communication in healthcare settings.
(2) Identify any ethical dilemmas presented in the scenario. Reflect on how ethical considerations impact decision-making in healthcare.
Your well-being is just as significant as that of the individuals you are caring for. It’s natural to experience intense reactions or emotions when discussing domestic violence, particularly if you have personally endured abuse or violence in the past or are presently facing it. Acknowledge your emotions and use this as a chance for self-reflection. Ensure you seek the necessary help and support for yourself.
Thought-provoking tasks for healthcare professionals
Preparation to identify and respond to domestic violence is paramount.
(1) How well prepared do you feel in this regard and what education and/or training resources are available to you or are you aware of in your area of practice? (2) Do you have a room in your clinical practice where you can speak to patients privately? (Behind curtains or screens is clearly not private or confidential). (3) In your area of practice, how might patients alert you that they wish to speak with you in private? (4) Do you currently have a clear referral pathway for patients to other services and support? (5) Do you know what services and supports are available for those who disclose domestic violence in your area of practice —and are contact details available to you? (6) Do you know how to make a referral to adult and children safeguarding services?
8. Visual Communication
Often, individuals experiencing domestic violence find it challenging to access information or support services. Visual communication plays a crucial role in raising awareness about domestic violence in medical settings such as hospitals and medical practices. Utilising tools like posters (e.g., with QR codes), leaflets, or pamphlets displays strategically placed in waiting rooms, bathrooms, and other visible areas is essential. Place information with support services in washrooms (with appropriate warnings about not taking them home if the perpetrator could find them).
These visual aids serve to communicate that the facility is a safe space for discussing domestic violence and make support services readily apparent. By creating a visual environment that openly addresses domestic violence, individuals are more likely to feel encouraged to speak up and seek help. This proactive approach contributes to breaking the silence around domestic violence and fostering a supportive atmosphere within healthcare settings.
Remember:
Use inclusive visuals that accurately represent the diverse experiences of individuals affected by violence (all genders without stereotypes).
If possible, use information available in multiple languages.
Choose impactful images that promote a positive message. Avoid harmful visuals such as depictions of physical violence (because DV is not only physical), sexualised portrayals of victim-survivors, and images exclusive to specific demographics.
Here are some examples on different tools:
Find tailored material for Germany, Sweden, Austria, Italy, Greece (coming soon).
Click here to see an example Video on how this sign is used in a video callwithout leaving a digital trace.
This is an international single-handed gesture used to draw attention to domestic violence. It can be employed when the person in need of help cannot speak loudly, for instance, because the perpetrator is nearby (in the car, at home etc.).
“The signal is performed by holding one hand up with the thumb tucked into the palm, then folding the four other fingers down, symbolically trapping the thumb by the rest of the finger.” 35
Leaflet
Distribute informational brochures about domestic violence awareness or local counselling services. Ideally, choose those that are in your vicinity and offer anonymous online counselling.
If it is not safe to give the affected person a flyer, it is a good option to create, for example, a business card with discreet phone numbers and addresses. You can see an example of a business card for men and women in the spotlight on dentistry.
Other
Buttons signalise that this is a safe space to talk about domestic violence.
Spotlight on Gynaecology/Obstetrics, Surgery & Paediatrics
9. Gynaecology/Obstetrics
Please watch this video featuring a health professional at an antenatal clinic conducting a screening for family and domestic violence. Pay close attention to the doctor’s communication style, observing how they engage with the patient through language, tone, and non-verbal cues. These elements are essential for building trust and rapport.
Task for reflection
(1) Evaluate the doctor’s ability to actively listen to Kaity’s concerns. Identify instances where active listening played a role in the interaction. (2) Consider the doctor’s approach in delivering sensitive information. How did she demonstrate empathy and sensitivity towards Kaity’s situation? (3) Reflect on any suggestions or support offered by the doctor for Kaity. How did the doctor address potential concerns or questions Kaity might have had?
„Have you ever been touched in a way that made you feel uncomfortable?“
„Has anyone ever made you to do something sexual when you did not want to?”
„Has your partner ever refused to practice safe sex?”
The following video showcases appropriate responses during a patient’s routine check-up. It emphasises essential aspects of patient care, particularly in creating a safe and comfortable environment for discussing sensitive topics. Focus on how the doctor thoughtfully introduces and addresses the subject of domestic violence, ensuring the conversation remains respectful and supportive throughout the consultation.
Task for reflection
(1) Assess whether the doctor’s communication reflected a patient-centred care approach. How did the doctor involve the patient in the decision-making process? (2) Pay attention to the doctor’s body language and non-verbal cues. How did these elements contribute to or impact the overall communication? (3) Summarise your overall impressions of the doctor’s communication style in this particular scenario. What stood out as particularly effective or areas that could be improved?
This example video features a young woman who receives a negative pregnancy test and wishes to discuss birth control options. It begins with a brief introduction to the topic of reproductive coercion. Pay close attention to how the doctor engages with the patient, offering guidance and support while addressing sensitive topics in a respectful and informative manner.
Task for reflection
(1) Identify moments where the healthcare provider expresses empathy and understanding towards the patient. How does this impact the patient’s experience? (2) Consider the cultural competence displayed by the healthcare provider. Are there instances where cultural sensitivity is evident in the communication? (3) Reflect on the strategies used by the healthcare provider to build and maintain trust with the patient. How important is trust in this healthcare setting?
Example on how to address domestic violence awareness in midwifery practice:
Due to pelvic discomfort, the midwife instructs Alessia to provide a urine sample. In the restroom of the midwifery practice, Alessia notices a poster with information and data on domestic violence, along with yellow adhesive dots attached to it. Next to these dots, Alessia reads the prompt, “If you would like to talk about domestic violence, please stick one of these dots under your urine container.” After some hesitation, Alessia takes a dot, affixes it under the urine container, and places it in the designated compartment.37
Seeking Care After Trauma: Challenges in Booking a Gynecologist After Rape (The Klingenbeck Case)
Task for reflection
(1) What are the main barriers the person experiences when trying to make a gynecologist appointment? (2) In what specific ways does past rape affect the person’s trust in medical professionals? (3) Why is trauma-informed care in a clinical setting so important?
10. Surgery, Emergency Room
Unfortunately, the busy clinical environments pose numerous challenges in recognising, addressing, and assisting a victim of domestic violence.
Task for reflection
(1) Reflect on the physician’s response to the patient’s asthma. How did the physician show empathy, and what cues in the patient’s language indicated there might be an underlying issue? (2) Consider the moment when the patient hesitated to talk about the problems in the relationship. How did the physician enhance trust and create a safe space for the patient to share the experiences?
Case study: Recognising and responding to suspected domestic violence
Robin has come to the Emergency room with a suspected fractured arm, cracked ribs and bruising around his neck.
Robin has seen the triage nurse. He told the nurse that his injuries are the result of a fall down the stairs in his flat. Because of the bruise marks around his neck, Dr Andersson is concerned that Robin may be a victim of domestic violence.
Robin: I feel like such a fool! I don’t know what happened, I just tripped at the top of the stairs. I will try to be more careful in the future. Will it take much time to get better?
Dr Andersson: Accidents happen, Robin. Let’s focus on getting you better. I’ve noticed you’ve been here a few times recently. Any particular reason?
Robin: I’m just very clumsy I suppose. I keep falling, you know?
Dr Andersson: But the bruising around your neck is a very unusual injury to sustain from a fall. It’s far more likely to have been caused by pressure being applied, perhaps from someone’s hands…? Is everything okay at home?
Robin: I don’t know what you’re suggesting but everything is just fine. Can you please just fix my arm and let me go home now?
Dr Andersson: I want to make sure you get the right care. Despite what you’re saying, I’m concerned about your injuries. Can you share more about what might be going on at home?
(Robin remains silent)
Dr Andersson: I’m here to help, Robin. If there’s something you’re not comfortable sharing, that’s okay. But it’s crucial for your well-being that we understand the full picture. Now, about these injuries, let’s figure out the best course of action for your recovery.
Robin: (begins to cry) You know, a new roommate moved in a couple of months ago. At first, it was just joking around, funny punches and all. But then it got worse, and he would hurt me. When he’s stressed from university, he takes it out on me. I think I might be depressed. I can’t talk to anyone; I’m scared and feel powerless.
Dr Andersson (pauses and gives Robin time to do so): I know this is difficult to talk about. I appreciate you sharing that, Robin. It’s not easy. You don’t have to go through this alone. It is not ok that your roommate is hurting you and you are afraid of him. It’s essential to address both your physical injuries and emotional well-being. I am really concerned about your safety and would like you to speak with a victim protection group or a specialised NGO.
Task for reflection
(1) Assess the doctor’s communication skills in this scenario. What techniques did Dr Andersson use to encourage Robin to open up about his situation? How can effective communication play a pivotal role in cases of potential violence? (2) Consider the cues that raised Dr. Andersson’s concerns about domestic violence. How did the doctor navigate this delicate situation while respecting Robin’s initial reluctance to share details? (3) Evaluate Dr. Andersson’s communication strategy. How did the doctor manage to persist in getting information about Robin’s injuries while being sensitive to his emotional state?
(1) Reflect on the manner in which the paediatrician conveyed information. What observations did you make regarding the choice of language and phrasing? (2) What else did you noticed in the setting?
Child abuse manifests in diverse forms, and its impact on each child differs. Not all cases involve visible injuries, making it crucial to explore indicators in Module 2. While physical harm may not be evident in most cases, the enduring effects on a child’s neurological, cognitive, and emotional development pose greater challenges. Discover more about the long-term impact of domestic violence on children, whether as witnesses or victims, here.
Talking about Sexual Violence – Could it also be that children make this up?38
It’s important to know that sexual actions by adults are not part of children’s experience. Therefore, it is highly unlikely that they would invent stories or develop “vivid fantasies” about it. Lies and imagination are typically children’s attempts to elevate themselves, to “make themselves important.” However, because sexual violence involves devaluation and shame, children usually do not make up such events. In rare cases, they may name a different person as the perpetrator, perhaps to protect perpetrators close to them. Sometimes, this happens because they are very afraid of him or her. It’s also possible that individual parts of their accounts may be incorrect, but the core information is still accurate.
This applies to teenagers as well, although sexual interactions with adults can be part of their experience. Unlike children, they may be more prone to inventing instances of sexual violence. At the same time, teenagers are well aware of the potential consequences they might face: teenage victims are often blamed and/or stigmatised. Therefore, very few teenagers, like children, fabricate situations to harm adults.
Both teenagers and children, who often have significant hurdles to overcome to communicate, deserve that we believe them, avoiding reflexive disbelief. The fear of not being believed is, by the way, one of the reasons why many choose to remain silent.
One of the greatest fears of children and adolescents who experience domestic/sexual violence within the family is that the family will fall apart if they start talking about it. They feel responsible for the family. It is even worse that this fear is often justified: They often have to endure the ignorance or accusations of other family members once they have found the courage to say what is or what was.
Such an evasive approach to survivors, however, turns responsibilities upside down. It is not the disclosure of domestic/sexual violence within a family that shakes the family to its foundations. The destruction occurred long before: namely, when a parent or another family member used the private sanctuary of the family, where children and all other family members should feel safe, secure, and familiar with each other, to initiate and perpetrate violence.
The concern about doing injustice to someone with a suspicion is widespread. Most false suspicions arise not because children or adolescents are lying but rather because adults quickly express suspicion when they find situations or specific behaviour peculiar or suspicious. Some people interpret changes in behaviour in children and adolescents as seemingly certain signs of domestic/sexual violence or misunderstand their statements. Some are so worried that they speak biasedly with children or adolescents, unintentionally prompting them to respond in a way that is supposedly expected of them.
At the same time, we must know that a suspicion cannot be resolved by confronting the suspected person. Both those wrongly accused and perpetrators equally deny such accusations. That’s why it’s so crucial for experienced professionals to talk to children and adolescents. They are best able to assess how to interpret the statements and whether a suspicion can be substantiated or, on the contrary, dispelled through these statements.
There are a range of reasons why children and young people do not disclose, even when there is physical evidence or an admission of offending by an alleged abuser. These include but are not restricted to:
the person who has experienced sexual abuse, or other family member, feeling guilty, fearful, embarrassed, or ashamed
a lack of language skills to communicate the abuse
a fear of not being believed
fear of retribution
afraid of threats made by the alleged abuser or a significant other
fear of things getting worse due to an adult’s intervention or past negative experiences
system and community responses, such as fear of what will happen following the disclosure
trauma – the severity of the abuse, being unable to remember the details of the abuse
dissociation, which can occur:
during the interview or engagement with the child, thereby restricting the practitioner’s ability to obtain information
during the abuse, which impacts the child’s ability to remember or articulate the memory of the abuse
inability to recognise the activity as abusive
cultural considerations (further outlined below)
not wanting to talk to strangers
the gender of the interviewer
lack of parental support, either explicitly voiced or implied
lack of confidence in adults and their ability to help.
Some children may choose not to communicate verbally about domestic violence, while others may indirectly disclose by hinting at the details or expressing it in a roundabout manner, such as saying, “sometimes my stepfather annoys my daddy” or “my aunt, who lives with us, screams a lot”. It is crucial to recognise and respond to these indirect disclosures.
Moreover, many children feel uncertain because the perpetrator is someone they love. Offer initial support that is gender-sensitive and focused on the child or adolescent. This involves: 42
listening respectfully and empathetically to the information that is provided;
inquiring about the child’s or adolescent’s worries or concerns and needs, and answering all questions;
offering a non-judgmental and validating response;
taking actions to enhance their safety and minimise harm, including disclosure and, where possible, the likelihood of the abuse continuing, this includes ensuring visual and auditory privacy;
providing emotional and practical support by facilitating access to psychosocial services;
providing age-appropriate information about what will be done to provide them with care, including whether their disclosure of abuse will have to be reported to relevant designated authorities;
attending to them in a timely way and in accordance with their needs and wishes;
prioritising immediate medical needs and first-line support;
making the environment and manner in which care is being provided appropriate to age, as well as sensitive to the needs of those facing discrimination related to, for example, disability or sexual orientation;
minimising the need for them to go to multiple points of care;
empowering non-offending caregivers with information to understand possible symptoms and behaviours that the child or adolescent may show in the coming days or months and when to seek further help.
Screening questions
Ask simple questions. The child should not be “interrogated”. Allow silences. If the individual cries, give enough time to recover.
Phrases to use
“Is there something you’re sad or worried about?”
“Some kids can get scared at home. What do you believe may scare them?”
“What happens at your house (or daycare) when people get angry?” 43
Do not use
“Is the mark on your arm a result of parental physical punishment?”
Building trust and showing empathy
This is how you can provide support through validation and empathy. The child should be reassured.
“You are worthy and deserving of a safe and happy life.”49
Do not use
“You should feel lucky you survived”
“Poor you”
It is ok to pause
Don’t pressure them to tell their story. Don’t look at your watch or speak too rapidly. Don’t answer the telephone, look at a computer or write. Don’t interrupt. Wait until they have finished before asking questions.
Phrases to use
“I am here”
Do not use
“Even though you feel uncomfortable, it is better to talk about it. So please answer my questions.”
Take the burden from the child/teenager
If the victim is not ready to talk about the situation, do not force it. Recognise the right time and let the victim know about it. Lay off the pressure.
Phrases to use
“What is going on in your house is not your fault.”50
“It’s OK to have mixed feelings about either or both of your parents/family members”.
Do not use
“You shouldn’t feel that way”
“Why do your parents fight?”
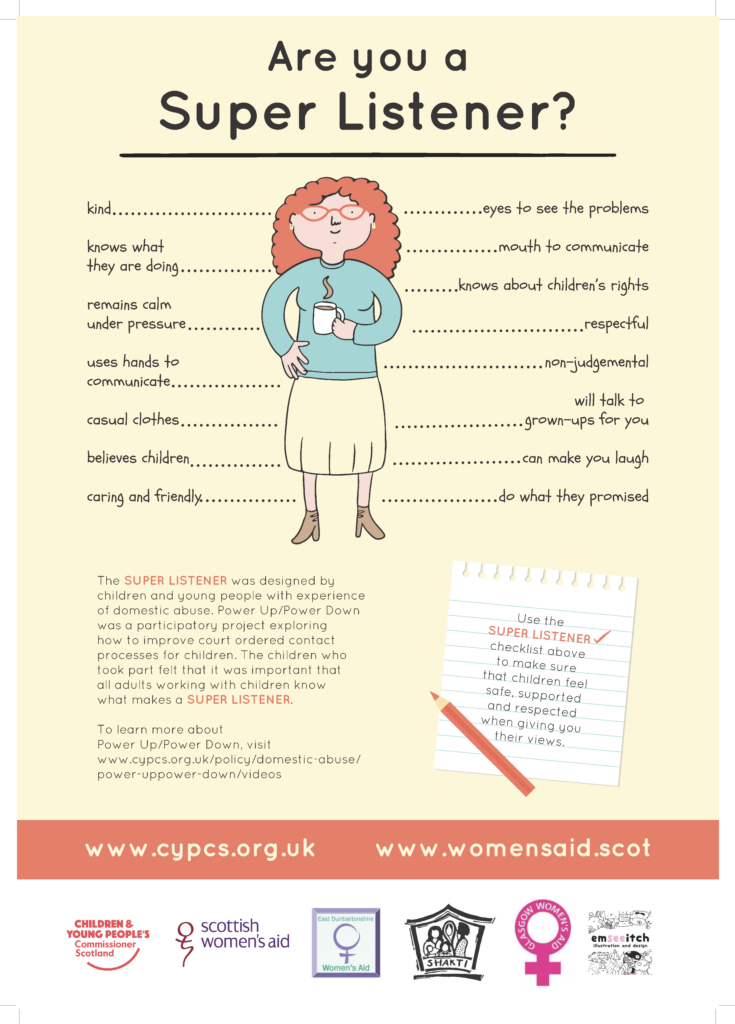
The SUPER LISTENER was designed by children and young people with experience of domestic abuse. Power Up/Power Down was a participatory project exploring how to improve court ordered contact processes for children. The children who took part in this programme felt that it was important that all adults working with children know what makes a SUPER LISTENER.
Please watch the video on how to support a caregiver who hasn’t disclosed domestic violence in a paediatric setting.
Task for reflection
(1) Observe instances where the healthcare provider demonstrates active listening skills. How does active listening contribute to effective communication in this scenario? (2) Assess how the healthcare provider delivers information to the patient. Is the information presented in a clear and understandable manner? (3) Observe how the healthcare provider addresses the patient’s concerns and questions. How effectively are these concerns addressed?
There are some good sources on how to communicate well with children being subjected to domestic and sexual violence:
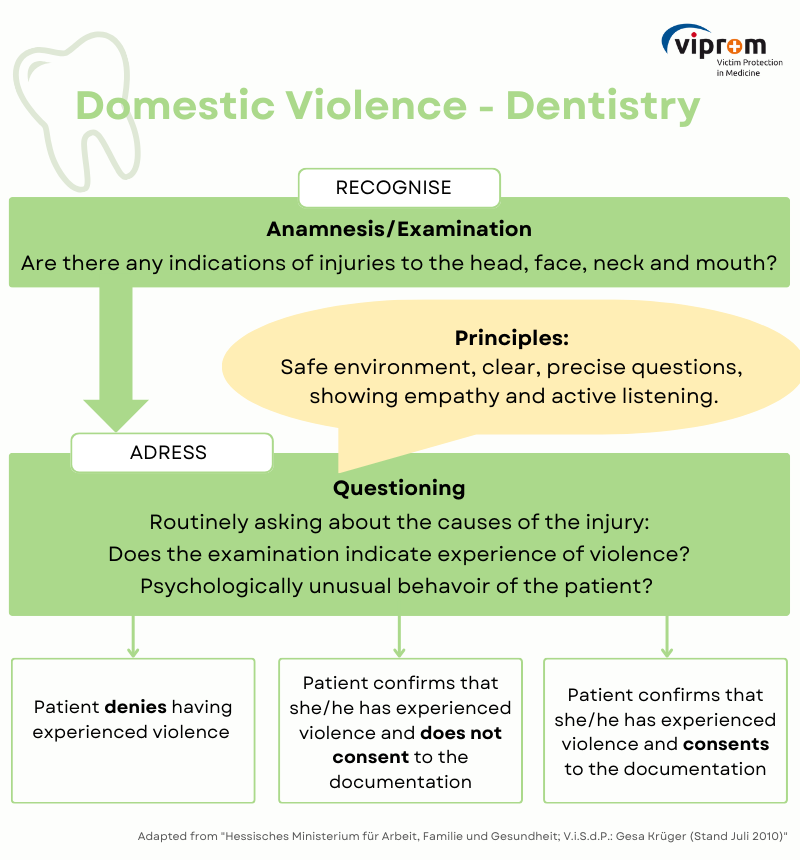
Case study: Recognising red flags and communication in a case suspecting violence in the dental practice
Mrs. Miller presents as a new patient at a dental practice. She comes in because of persistent toothache in her upper jaw. The dentist immediately notices the patient’s anxious and timid behaviour. Although the patient has already filled out a medical history form in the waiting room, the dentist takes a moment to get to know the patient better.
Dentist: “Have you recently moved to K., Mrs Miller?”
Mrs Miller: “No, my husband and I have lived here for seven years. I haven’t had any problems with my teeth yet. But now my toothache is giving me such sleepless nights that it’s unbearable.”
Dentist: “OK, then I’ll take a closer look”. At the start of treatment, the dentist recognises a small reddish haemorrhage around the patient’s eyes.
When she tries to look into Mrs Miller´s mouth with her mirror, the patient immediately flinches away. “I’m being very careful,” she says to the patient. “I’m just trying to get an overview to understand where the pain could be coming from”.
Mrs Miller nods, but her body does not relax. The cramped posture remains. When Mrs Miller is startled during the examination, her scarf slips and the dentist sees several dark purple and already faded haematomas at her neck. The dentist notices it, but doesn’t give it a second thought.
As the dentist cannot see where the toothache is coming from during the examination, she orders an X-ray. “Is that really necessary?” asks Mrs Miller. “Yes, definitely,” replies the dentist. “This is your first visit today. I would like to get an overview. Root tips and possible inflammation can only be diagnosed with an X-ray. To do this, I would like to take an overview image (OPG/PSA) showing all the teeth, the jaws and both temporomandibular joints. Furthermore, I cannot clearly see from the external examination where exactly your pain is coming from, i.e. from which tooth. Unfortunately, I can’t help you without having more Information. An X-ray is not painful at all. The machine only goes around you once!”.
When the dentist sees the x-ray, she is shocked. She recognises a fracture of the lower jaw on the x-ray. She wonders why Mrs Miller didn’t come earlier. That must have been hellish pain. When Mrs Miller is back in her treatment chair, the dentist mentions the broken jaw.
Dentist: “I can see a fresh fracture of the lower jaw on the x-ray, which may be responsible for the pain. Do you remember how this injury occurred?”
Mrs. Miller replies: “Oh, that was a long time ago. I can’t really remember it anymore.”
Dentist: “Is everything fine at home? Such injuries often occur when someone has been hurt by someone. Was that the case with you? I also saw several bruises on your neck.”
Mrs. Miller´s eyes fill with tears, but she doesn’t answer the questions. The dentist respects this and doesn’t want to put pressure on her.
At the end of the treatment, however, the dentist gives her a sort of a business card with the hidden numbers of women’s shelters and violence hotlines and explains that she can go there if something at home frightens her or she doesn’t feel safe any longer. She is also welcome to get in touch with her, too in case of need and tells her that nobody is allowed to hurt or frighten another person.
The dentist promptly calls the patient back in to continue the treatment and makes a corresponding note in the patient’s file. She plans to speak to Mrs. Miller again about the situation at home.
Task for reflection
(1) What indicators can be identified in this case study that Mrs. Miller could be a victim of domestic violence? (2) What type of questions did the dentist ask the patient – direct or indirect? (3) What worries and fears might patients such as Mrs. Miller experience in the dental practice? What could prevent victims from disclosing the domestic violence they have experienced? (4) How did the dentist react when Mrs Miller did not answer the questions about domestic violence?
Possible reasons why victims do not speak up about domestic violence in the dental practice: 51
Information on screening on domestic violence can be included directly in the medical history form e.g. “We generally ask our patients about domestic violence!”
The better dentists know how they can help those affected by domestic violence and the more knowledge they have about it in general, the more confident they will feel about raising the issue.
Posters can be put up in the waiting room and information leaflets can be displayed. For more information see 8. Visual Communication.
If it is not safe to give the victim a flyer, it is a good option to design a business card, for example, with concealed numbers and addresses. In this example, a business card was designed for men and one for women, containing information on support centres in the Münster (Germany) area.
The numbers have been anonymised for safety reasons and to protect the individuals involved. Please check with the relevant authorities in your area and insert the correct numbers.
Two business cards can be created: one for women that includes relevant numbers such as women’s shelters, and another for men listing men’s shelters and similar services. This approach will better support those in need and reduce the barrier to contacting the appropriate counselling services.
Levinson W, Gorawara-Bhat R, Lamb J. A Study of Patient Clues and Physician Responses in Primary Care and Surgical Settings. JAMA. 2000;284(8):1021–1027. doi:10.1001/jama.284.8.1021 ↩︎
Trauma-Informed Care Implementation Resource Center, https://www.traumainformedcare.chcs.org/what-is-trauma-informed-care/, accessed 11.01.2024 ↩︎
Trauma-Informed Care Implementation Resource Center, https://www.traumainformedcare.chcs.org/what-is-trauma-informed-care/, accessed 11.01.2024 ↩︎
“What Is Patient-Centered Care? Explore the definition, benefits, and examples of patient-centered care. How does patient-centered care translate to new delivery models?” NEJM Catalyst, January 1, 2017, accessed 11.02.2024. https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0559↩︎
“A National Protocol for Intimate Partner Violence Medical Forensic Examinations”, U.S. Department of Justice Office on Violence Against Women, May 2023, p. 20, accessed 11.01.24. ↩︎
“A National Protocol for Intimate Partner Violence Medical Forensic Examinations”, U.S. Department of Justice Office on Violence Against Women, May 2023, p. 21, accessed 11.01.24. ↩︎
“A National Protocol for Intimate Partner Violence Medical Forensic Examinations”, U.S. Department of Justice Office on Violence Against Women, May 2023, p. 21, accessed 11.01.24. ↩︎
Rhodes KV, Frankel RM, Levinthal N, Prenoveau E, Bailey J, Levinson W. “You’re not a victim of domestic violence, are you?” Provider patient communication about domestic violence. Ann Intern Med. 2007 Nov 6;147(9):620-7. doi: 10.7326/0003-4819-147-9-200711060-00006. PMID: 17975184; PMCID: PMC2365713. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Rhodes KV, Frankel RM, Levinthal N, Prenoveau E, Bailey J, Levinson W. “You’re not a victim of domestic violence, are you?” Provider patient communication about domestic violence. Ann Intern Med. 2007 Nov 6;147(9):620-7. doi: 10.7326/0003-4819-147-9-200711060-00006. PMID: 17975184; PMCID: PMC2365713. ↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT, & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509 ↩︎
[1] Ashur M. L. (1993). Asking about domestic violence: SAFE questions. JAMA, 269(18), 2367. ↩︎
Translated and adapted from Schäfers, R. (2012). Gesundheitsförderung durch Hebammen: Fürsorge und Prävention rund um Geburt und Mutterschaft (1st ed.). Schattauer. p. 127. ↩︎
Bundesministerium für Familie, Senioren, Frauen und Jugend (BMFSFJ) und der Unabhängigen Beauftragten für Fragen des sexuellen Kindesmissbrauchs (UBSKM), Kampagne: “Nicht wegschieben”, accessed 12.01.2024. https://nicht-wegschieben.de/informieren↩︎
Bundesministerium für Familie, Senioren, Frauen und Jugend (BMFSFJ) und der Unabhängigen Beauftragten für Fragen des sexuellen Kindesmissbrauchs (UBSKM), Kampagne: “Nicht wegschieben”, accessed 12.01.2024. https://nicht-wegschieben.de/informieren↩︎
Bundesministerium für Familie, Senioren, Frauen und Jugend (BMFSFJ) und der Unabhängigen Beauftragten für Fragen des sexuellen Kindesmissbrauchs (UBSKM), Kampagne: “Nicht wegschieben”, accessed 12.01.2024. https://nicht-wegschieben.de/informieren↩︎
World Health Organization. (2017). Responding to children and adolescents who have been sexually abused: WHO clinical guidelines. World Health Organization. P. 18-19. https://www.who.int/publications/i/item/9789241550147↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Thackeray, J., Livingston, N., Ragavan, M. I., Schaechter, J., Sigel, E., COUNCIL ON CHILD ABUSE AND NEGLECT , & COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION (2023). Intimate Partner Violence: Role of the Pediatrician. Pediatrics, 152(1), e2023062509. https://doi.org/10.1542/peds.2023-062509↩︎
Femi-Ajao, O. (2021). Perception of Women with Lived Experience of Domestic Violence and Abuse on the Involvement of the Dental Team in Supporting Adult Patients with Lived Experience of Domestic Abuse in England: A Pilot Study. International journal of environmental research and public health, 18(4). https://doi.org/10.3390/ijerph18042024↩︎